
John Paul Gallardo, D.D.S., P.A., Periodontics and Implant Dentistry
From Our Office
to Yours….
The design of implant-supported tooth restorations plays a key role in maintaining peri-implant health.
A 2025 study by the American Academy of Periodontology and the Academy of Osseointegration examined how different design features of implant-supported tooth restorations impact oral tissue health.
The study concluded that poorly conceived prosthetic designs contribute to peri-implantitis and marginal bone loss.
This current issue of The PerioDontaLetter addresses the designs which have been shown to have a connection with peri-implantitis and marginal bone loss, and how careful implant-supported prosthetic design can improve long-term oral health, reduce complications, and maintain stability around dental implants.
As always, we welcome your comments and suggestions.
The Influence of Prosthetic Designs On Peri-Implant Bone Loss
Peri-implantitis and marginal bone loss (MBL) have been associated with certain prosthetic designs, particularly those which contribute to plaque deposition.
A growing body of evidence now establishes substantial connections between implant prosthetic design, biofilm accumulation, and peri-implant health.
The American Academy of Periodontology (AAP) along with the American Academy of Osseointegration (AO) undertook a review of research published over the 43 years between 1980 and 2023 on the impact of prosthetic design on peri-implant health.
Published in 2025, their study illuminates the critical aspects of implant-supported prosthetic designs which contribute to peri-implant marginal bone loss (MBL).
These critical aspects include:
- Platform-switched and platform-matched designs
- Abutment height
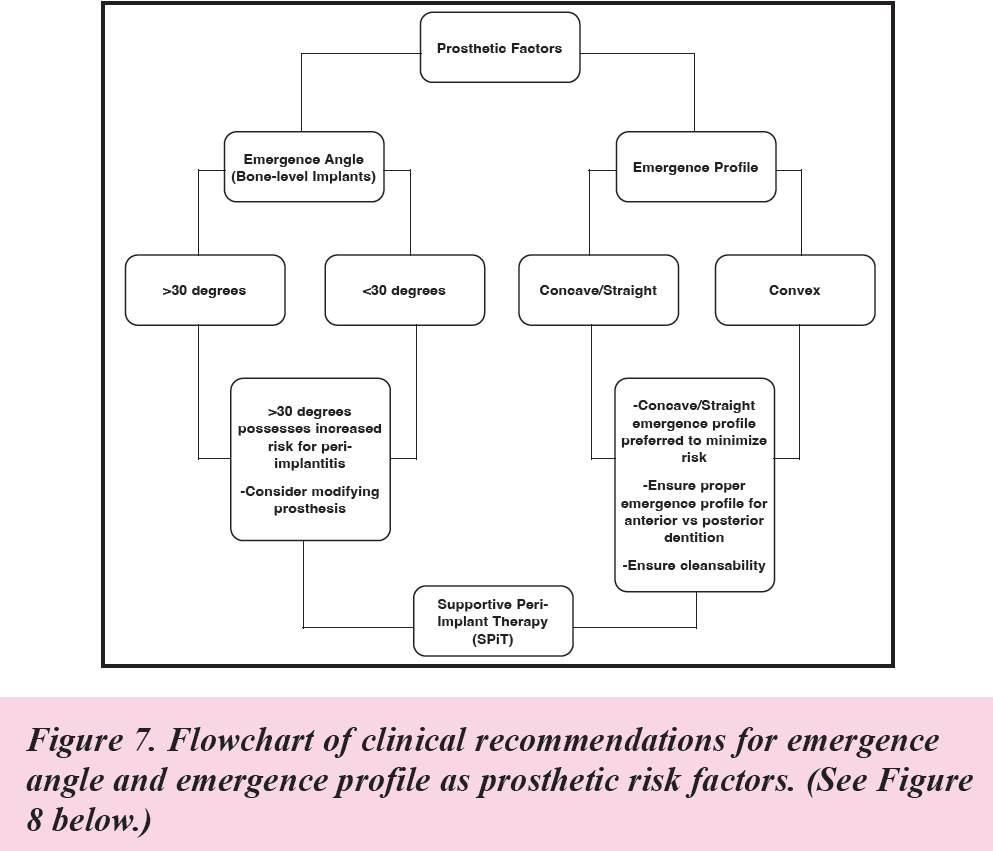
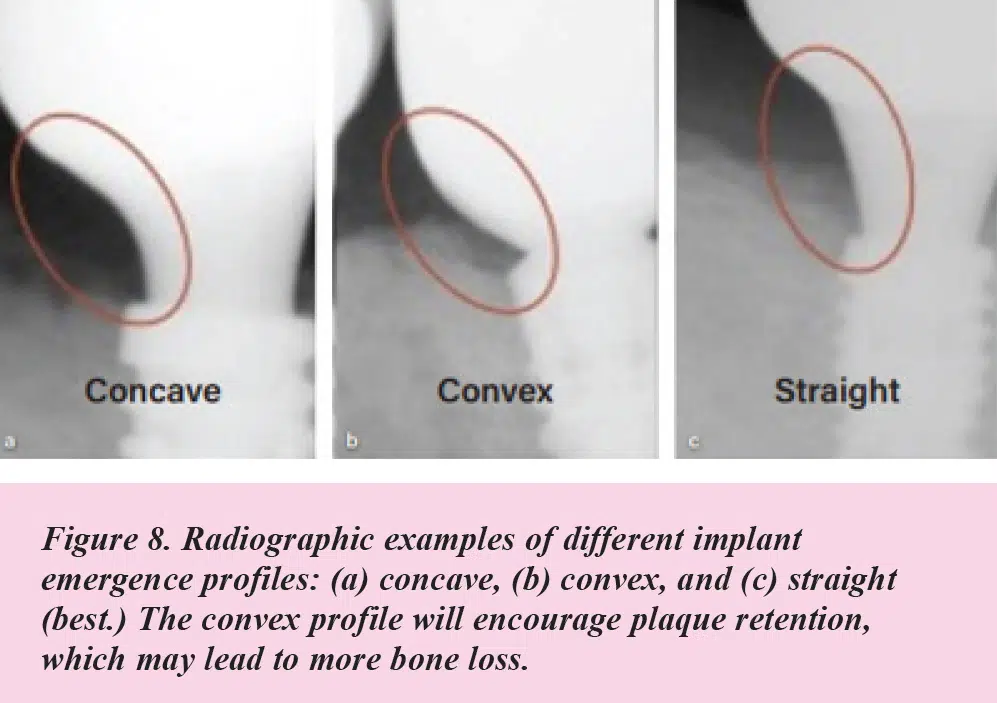
- Emergence angle and profile (See Figure 8)
- Implant-abutment connection type (See Figure 1.)
- Splinted vs. non-splinted restorations (See Figures 5 and 6)
- Frequency of abutment disconnections

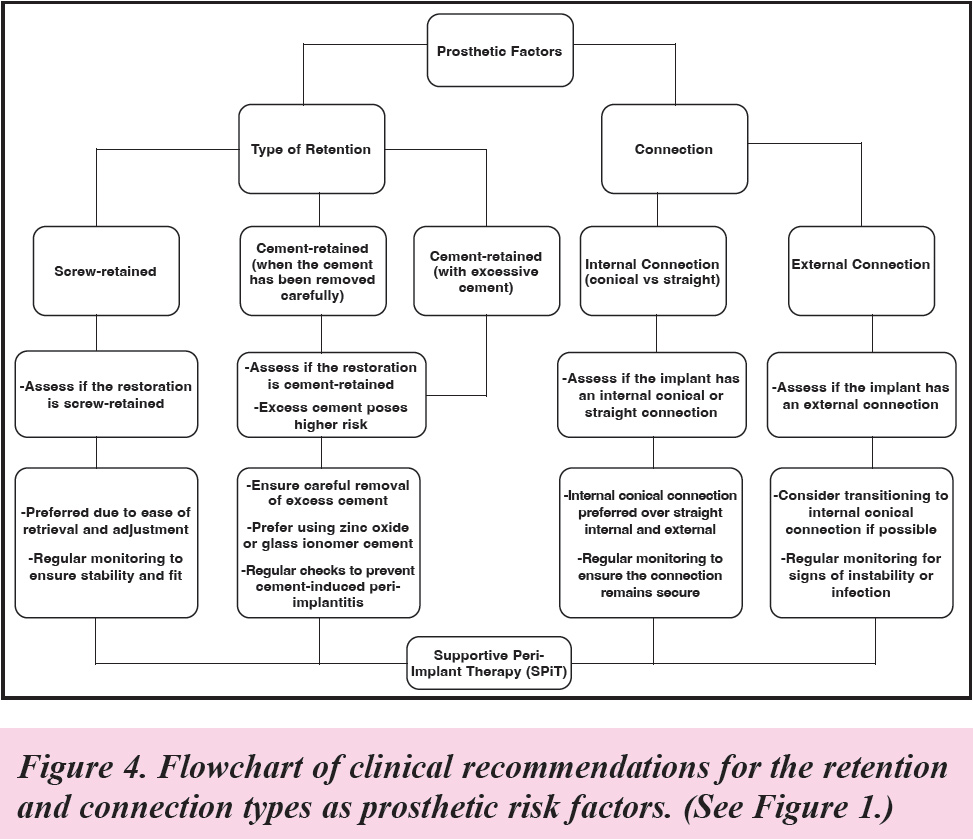
No significant difference between screw-retained prostheses and cement-retained prostheses was demonstrated in MBL when the cement was carefully removed.
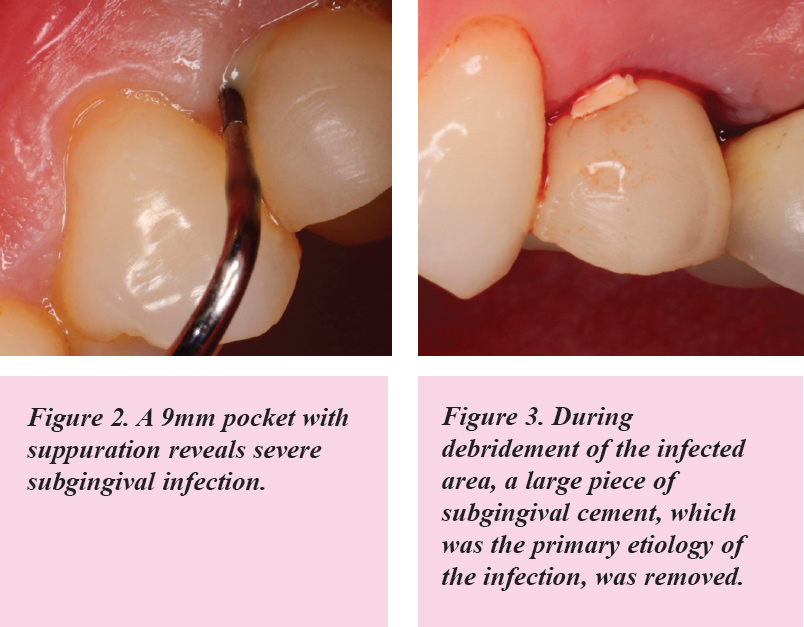
There is significant evidence that residual cement is a major factor causing peri-implantitis; so it is critical to be careful that the cement is “cleaned” around an implant prosthesis, or it will likely contribute to plaque retention, which in turn contributes to peri-implantitis. (See Figures 2 and 3.)
Several techniques have been introduced to effectively and completely remove or reduce residual cement. Additionally, the use of water-soluble zinc oxide cement, glass ionomer cement, radiopaque resin cement, and magnification or refining the finish line to be more biologically oriented.
No significant connection was shown between the crown-to-implant ratio and the development of MBL.
Platform Design
The implant-abutment interface is an area where peri-implantitis can develop. The risk is greatly influenced by whether the implant system uses a platform-switched or platform-matched design.
The AAP/AO Report found platform-switched abutments (where the abutment has a smaller diameter than the implant platform) have demonstrated a reduced risk of peri-implant bone loss by shifting the inflammatory response away from the implant shoulder.
Abutment Height
Abutment height is another key determinant in peri-implant health, particularly in relation to soft tissue support and plaque control.
Abutment heights < 2 mm may lead to crestal bone remodeling, as shorter abutments do not provide sufficient vertical space for healthy soft tissue attachment to form. In contrast, abutments with heights ≥ 2 mm are typically preferred, as they allow for adequate soft tissue adhesion, which helps protect the peri-implant area from bacterial penetration.
Additionally, shorter abutments can lead to severe crown emergence profiles, which create spaces where bacteria can accumulate and in turn make it harder for patients to maintain good hygiene around the implant.
Emergence Profile
According to the AAP/AO Consensus Report, the emergence angle and profile of an implant restoration is another critical determinant of peri-implant health, as it affects the ability of patients to maintain effective oral hygiene around the implant.
Emergence angles <30° and a concave/straight profile led to a lower risk of peri-implantitis.
Emergence angles >30 degrees were identified as high risk due to the difficulty in accessing and cleaning these areas, which can lead to increased plaque accumulation.
The Report found a convex emergence profile is particularly problematic as it creates undercuts where plaque can easily accumulate, exacerbating the risk of peri-implant inflammation and bone loss.
A thorough assessment of the emergence profile during prosthesis planning and fabrication stages is necessary to minimize these risks. (See Figure 9.)
Implant Abutment Connection
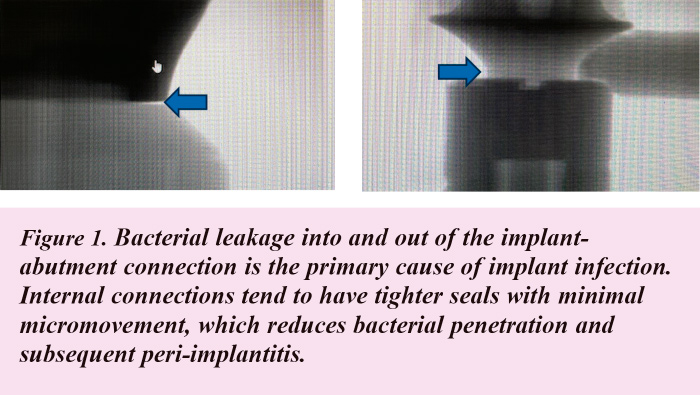
The implant-abutment connection type also plays a critical role in peri-implant health the report concluded. (See Figure 1.)
The Report found internal connections tend to have tighter seals at the implant-abutment interface, which reduces the risk of bacterial penetration and subsequent peri-implantitis.
External connections are more prone to mechanical complications, such as screw loosening, and they create larger microcaps where bacteria can accumulate, leading to a higher risk of peri-implantitis.
The Report concluded external connections may still be used in specific cases where the implant system requires them, but they necessitate more careful monitoring and maintenance. (See Figure 1.)
Splinted & NonSplinted Restorations
According to the Report, splinted vs nonsplinted restorations also factor into the risk for peri-implantitis and marginal bone loss.
Splinted restorations offer better stability in full-arch restorations, but potentially increase the risk of biofilm buildup if not designed with adequate spacing to facilitate oral hygiene efforts.
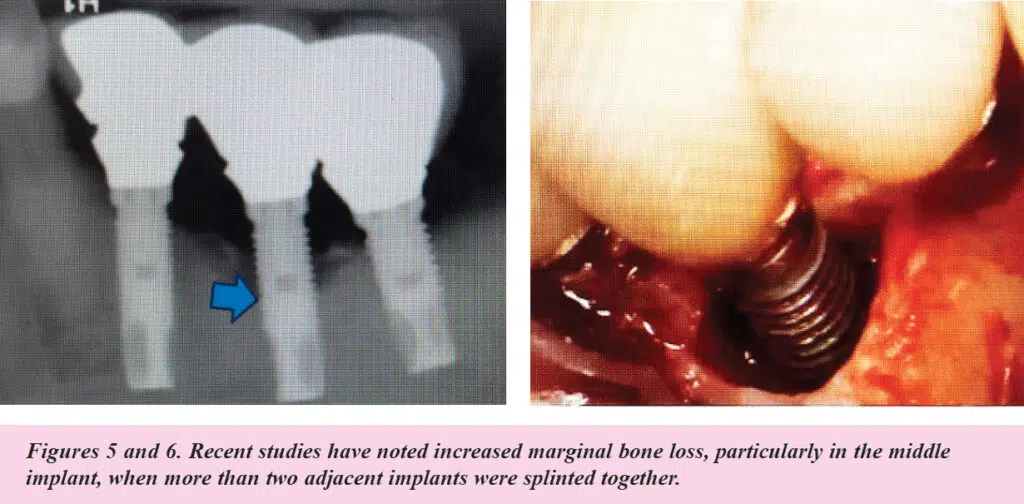
Recent studies cited by the AAP/AO also noted increased marginal bone loss, particularly in the middle implant, when three adjacent implants were splinted together. (See Figures 5 and 6.)
Frequency of Abutment Removal
Several other factors related to the abutment can increase the risk of peri-implantitis, including the frequency of abutment removal, which can break the soft tissue seal around the implant, leading to bacterial colonization and inflammation.
Multiple transmucosal components, including healing abutments, impression coping, provisional abutments, and final abutments, are routinely disconnected and reconnected throughout the treatment process. Findings cited in the Report revealed that a “one abutment-one time” protocol, which entails connecting the definitive abutment at the time of implant placement surgery, resulted in less MBL compared to repeated abutment disconnections.
The use of CAD/CAM custom abutments is preferred, as they provide a more precise fit and better tissue support compared to standard/stock abutments.
Additionally, large gaps between the implant and abutment connections, or misalignment during abutment placement, can create niches for bacterial growth, increasing the risk of peri-implantitis.
Achieving long-term peri-implant health necessitates not only optimal prosthetic designs but also the implementation of a well-structured maintenance protocol and the provision of comprehensive home care instructions for patients.
Conclusion
Clinicians strive to deliver implant restorations which are esthetic, functional, and biocompatible, which in turn will help patients achieve peri-implant tissue stability.
With careful consideration of the design features of implant-supported prostheses and their impact on peri-implant health, clinicians can reduce the risk of peri-implant disease potentially leading to peri-implant bone loss and unfavorable outcomes.